Pancreatic Cancer
Pancreatic Cancer Q & A
The pancreas is an organ which lies behind the stomach. It is anatomically divided into the head, neck, body and tail.
It has two major roles – the control of blood sugar by producing insulin and food digestion by producing digestive enzymes.
Pancreatic cancer (pancreatic ductal adenocarcinoma) arises from the part of the pancreas that produces digestive enzymes (the exocrine part).
This is different from tumours that occur in the part that produces hormones such as insulin (the endocrine part).
Pancreatic cancer is the ninth commonest cancer affecting just over 8000 people in the UK each year.
It is not clear what causes pancreatic cancer. Some of the risk factors include smoking and chronic (prolonged) inflammation of the pancreas (pancreatitis).
Excessive alcohol intake is a common cause of pancreatitis. Familial pancreatitis and certain familial cancers of the breast and bowel are also associated with a higher risk.
The symptoms depend on the location on the cancer. When the cancer is in the pancreatic head, which is the commonest site for cancer, it can block the bile duct, causing jaundice (yellowing of the skin), dark urine, pale stools, and itchy skin.
When the cancer obstructs the pancreatic duct, it prevents the flow of digestive enzymes, resulting in an inability to digest fat in food. This leads to bulky offensive stools that are difficult to flush. The inability to digest food effectively causes weight loss.
There may also be abdominal or back pain, nausea and loss of appetite. Some patients may present with symptoms of diabetes. Cancer in the body and tail of pancreas usually causes abdominal or back pain and weight loss.
Unfortunately most pancreatic cancers present at an advanced stage. Occasionally pancreatic tumours are picked up on a scan which is done for another reason.
Blood tests are usually performed to confirm the presence of jaundice. This is followed by an ultrasound scan and a computerised tomography (CT) scan. Occasionally a magnetic resonance imaging (MRI) scan is performed.
In most cases, it is necessary to obtain a small sample of tissue (biopsy) from the pancreas to confirm the diagnosis. If jaundice is present, then this often needs to be treated by draining the bile duct.
This is done by a procedure called endoscopic retrograde cholangiopancreatography (ERCP), which involves passing a flexible tube (endoscope) through the mouth. The endoscope is used to obtain samples from the tumour and to place a plastic tube (stent) to help drain the bile across the site of the blockage. Tissue from the tumour can be obtained at the same time.
Another procedure that can be used to obtain tissue samples is endoscopic ultrasound. This involves using a flexible endoscope with an ultrasound probe at the end, which allows a close examination of the pancreas and maps out the relation of the tumour to major blood vessels in the vicinity. A fine hollow needle is used to extract a biopsy from the tumor to confirm the diagnosis.
For every 100 patients with cancer of the pancreas, less than 20 can have their cancer surgically removed. In the rest the cancer is too advanced for surgery to be beneficial.
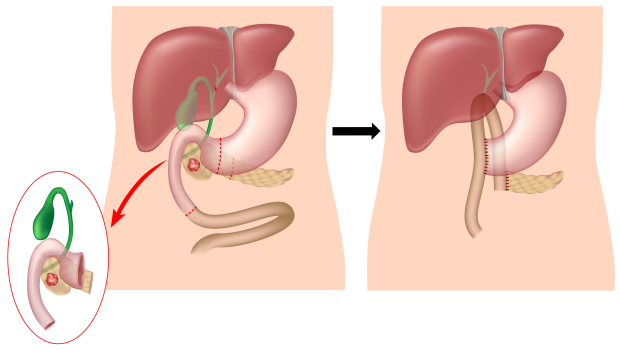
Whipple’s operation (pancreatico-duodenectomy) is usually performed to remove tumours in the head of pancreas (the operation is also performed for cancers arising in and around the ampulla, distal bile duct and duodenum).
This involves the removal of the pancreatic head together with the duodenum (the first part of the small bowel) and a short length of stomach and small bowel. The gallbladder and part of the bile duct are also removed.
The remaining pancreas, the bile duct and stomach are then connected to the small bowel to restore the gastro-intestinal continuity. This complex operation usually requires a hospital stay of 1-2 weeks.
The Whipple’s Procedure:
Tumours arising in the body or tail of the pancreas are removed by an operation called distal pancreatectomy which usually involves removal of the spleen (splenectomy) as well as the part of pancreas affected by the tumour.
Chemotherapy is recommended after surgery in most cases. This may be as part of a clinical trial testing different regimens of chemotherapy.
Radiotherapy in combination with chemotherapy is occasionally used to shrink advanced tumours that have not spread.


Pancreatic Neuroendocrine Tumours
Pancreatic Neuroendocrine Tumours Q & A
Pancreatic Cysts and Pseudocysts
Bile Duct Cancer Q & A
